Figure 7: Round cell sarcoma in a 22-month-old female rat (Agnes).
Case history and photos
History
Agnes, a SPF MYCO free, intact, retired female Sprague Dawley PEW lab rat, weighing 371 grams was born February 21, 2010, and not used in any experiments, was adopted by the present owner at four weeks of age along with the mother and siblings in March 2010. There were no signs of illness until November of 2011.
Clinical Signs
A wellness exam performed on October 15, 2011 showed that Agnes appeared healthy with no abnormalities
On November 15, 2011 the owner noted a visible lump on the outside edge at the back of the right hip. Agnes was again seen by the veterinarian and surgery was scheduled for November 18, 2011.
Diagnosis
Subdermal firm mass over R hip,
Treatment
On November 18, 2011, Agnes underwent surgery to remove the mass over the right hip. The mass, suspicious for cancer, was then sent for histopathology.
Postop recovery was uneventful. Pain was managed well with buprenorphine given at time of surgery, and Metacam given postop. Arrangements were made by the owner to pick Agnes up the following evening.
Home care detailed cage rest and limited activity for a week and to return for re-exam if there were any concerns.
During home recovery, Agnes and her sister, Darlene (who had undergone a mammary tumor removal and spay the day before), were housed in a one level cage, on newspaper and paper towels with fleece, along with a cardboard cereal box to hide in. Bedding was changed completely each night. They remained housed in a one level cage throughout the healing process for 14 days.
Nutrition for Agnes and Darlene throughout the recovery process consisted of:
- Envigo (Formerly Harlan Teklad) 2014 and Oxbow Regal Rat pellets provided free choice.
- Nightly offered two tablespoons of table food that was a mix of cooked broccoli, mashed sweet potatoes, and vegetables from homemade chicken soup with broth.
- A teaspoon of Ensure twice a day during the first week of recovery to help with hydration.
Outcome
Over the course of a couple of weeks Agnes seemed to heal beautifully and at that time there was no notice the mass on her hip was returning.
A histopathology report of the removed mass showed the following:
Biopsy
MICROSCOPIC FINDINGS:
Round cell tumor (round cell sarcoma), with multifocal necrosis, right hip
COMMENTS:
The most accurate diagnosis for this lesion is a round cell tumor or round cell sarcoma. Some of these cells
with more voluminous pale-staining cytoplasm and occasional fine, sparse granularity are vaguely reminiscent of mast cells. Therefore, a special stain will be performed to attempt identification of possible mast cell granules and therefore a more specific tumor classification. An addendum to this report will follow to relate the results of a special stain procedure.
************ ADDENDUM COMMENTS – 12/03/11 ************
ADDENDUM FOR SPECIAL STAINING:
Special staining for mast cells using the Giemsa procedure it is negative. Although this fails to confirm a poorly differentiated mast cell tumor, it still does not totally rule out this possibility since undifferentiated mast cells with no intracytoplasmic granularity are negatively staining. Other differential diagnostic considerations include an unclassified round cell sarcoma or a round cell tumor of plasmacytic or lymphoreticular origin. The lesion is locally infiltrative, and the neoplastic cells extend to and form all margins of the specimen.
Follow-up
On the evening of December 19th Agnes was sluggish and unable to eat much.
She died at home during the day of December 20th before she was to be taken for supportive veterinary care.
Necropsy and histopathology report as follows:
Necropsy:
Liver is greatly enlarged – suggestive of metastatic disease? Lungs are spotty with appearance of hyperemic areas – possibly post mortem. There appears to be regrowth of the original cancer.
- Focally disseminated metastatic neoplasia
(poorly-differentiated sarcoma) - Moderate to marked, diffuse microvascular congestion
- Mild pulmonary edema
Biopsy
CLINICAL HISTORY:
Multiple tissues derived by necropsy performed on a mature adult rat are submitted with the clinical history of a previous round cell sarcoma localized to the thigh. The patient died one month post-operatively.
MICROSCOPIC DESCRIPTION:
The kidney is histologically unremarkable, maintaining normal tubuloglomerular microstructure with no interruption in renal parenchymal integrity by inflammation, necrosis/infarction, or neoplasia. There is moderate congestion of the microvasculature existing at the corticomedullary interface.
Glomeruli are devoid of excessive mesangial cellularity or thickening of glomerular capillary basement membranes. Tubules are devoid of casts of proteinaceous or other variety. There is no interstitial nephritis or fibrosis, glomerulonephritis, or pyelonephritis.
Liver is characterized by partial severe effacement of pre-existing hepatocellular plate and sinusoidal microstructure by multiple independent to confluent foci of acute coagulative to liquefactive necrosis. Independent foci of necrosis isolate foci of intact upon sites, the latter appearing with some uniformity around the portal areas, suggesting that the necrosis is predominantly centrilobular. The necrotic foci are characterized by the complete dissociation of hepatocellular plates and hepatocellular drop-out or obsolescence. Subsequently the sinusoids have become confluent to create pools of blood within the necrotic foci. Section of the neoplasm is a compactly, solidly cellular, monotonous sheet of pleomorphic mesenchymal cells. Cytomorphology includes ovoid, polyhedral, and laterally flattened shape with round to ovoid nuclei of variable size and chromatin distribution. The latter includes occasionally condensed chromatin which creates an hyperchromatic appearance or marginated chromatin which contributes to an open-faced/vesicular appearance and exposes nucleoli variable from solitary and large to multiple and small. No mitotic figures are observed. The neoplasm also contains foci of acute coagulative to liquefactive necrosis devoid of secondary inflammatory infiltrates. There are no characteristic cellular organizational patterns or cytologic features.
Lung is characterized by multiple foci of the pleomorphic neoplastic foci scattered randomly and haphazardly as well as multifocally circumscribing small-caliber pulmonary arterioles and venules.
Considered collectively, the multiple foci of metastatic mesenchymal cells occupy an estimated approximation of one-third to one-half of the pulmonary cross-sectional surface area. The interalveolar septal microvasculature is moderately-congested. Alveoli are devoid of stainable fluid content but contain occasional macrophages (indirect evidence of pulmonary edema).
MICROSCOPIC FINDINGS:
Kidney- no microscopic lesions
Liver- severe, acute coagulative to liquefactive necrosis
Mass- poorly differentiated malignant mesenchymal tumor (sarcoma)
Lung-
-
COMMENTS:
It is presumed that the specimen representing the neoplasm is a sample of residual or recurrent neoplasm which was originally identified within the thigh. Since the neoplastic mesenchymal cells are more commonly of ovoid to angular to polyhedral rather than attenuated/fusiform morphology, the neoplasm is properly sub–classified as a “round cell” sarcoma. However, the exact histogenesis (specific cell type of origin) is undetermined due to poor cellular differentiation and organization. The neoplasm has metastasized to the lung. In addition to the primary and metastatic neoplasm, there is also a significant but non-neoplastic hepatic lesion (multifocal acute necrosis). The relationship between the neoplasm and the hepatic necrosis is questionable, but it is possible that pulmonary functional compromise due to significant replacement of pulmonary parenchyma by the neoplasm has resulted in hypoxic hepatic necrosis (?).
Synopsis
Cause of death: metastasis of cancer to the lungs with resultant disease and necrosis of the liver.
Photos
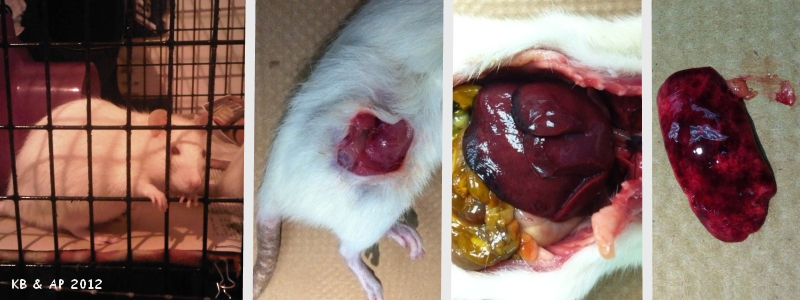 Photo 1 shows a healthy Agnes. Photo 2 taken at time of necropsy shows site where mass was previously located. Photo 3 shows liver necrosis. Photo 4 shows kidney with no significant microscopic lesions. |
Veterinary surgeon: Anthony Pilny DVM, DABVP
Necropsy and Synopsis: Anthony Pilny DVM, DABVP
Pathologist for both biopsy reports: Ken Mero, DVM, PhD
Photos: Anthony Pilny DVM, DABVP and Karen Borga
Case history courtesy of Karen Borga.

